https://doi.org/10.18593/evid.34517
Individuals with Temporomandibular Dysfunction show reduced strength of the cervical muscles
Indivíduos com Disfunção Temporomandibular apresentam redução da força dos músculos cervicais
Thayllane Costa Cardoso1; Daniela Bassi Dibai2, Josmayara da Silva Caldas3; Ana Lívia Oliveira4, Camila Vitória de Moraes Costa5; Kelyanne dos Santos Pinho6; Maria Ticiane Ferreira Marques7; Maria Claudia Gonçalves8
Abstract: Introduction: The literature indicates that individuals with temporomandibular disorder (TMD) also present pain and changes in the posture of the cervical spine, but there are still few studies that have evaluated the strength of the cervical muscles. Objectives: To evaluate cervical muscle strength in young adults with and without temporomandibular disorders. Materials and Methods: Young adults aged 18 to 25 years from a private university, with and without a diagnosis of TMD and in good general health, participated in this study. Individuals with neck/head trauma were excluded; disc herniation and degeneration; systemic diseases such as fibromyalgia, lupus; pregnancy; anesthetic block during the last 3 months. Questionnaires with general data and the Fonseca Anamnestic Index were applied to evaluate the signs and symptoms of TMD and Neck Disability Index (NDI) to assess the level of disability related to pain in the cervical spine. The assessment of muscular strength of the cervical flexor and extensor muscles measured by maximal isometric voluntary contraction (MVIC) was performed using a manual dynamometer, model 2201163, Lafayette, IN, USA. Results: A higher frequency of signs and symptoms of moderate TMD was observed (53%). A reduction in muscle strength in the TMD group was identified in relation to the group without TMD for all movements, but a significant difference was observed only in the flexion movement. Conclusion: Individuals with TMD have lower muscle strength for all movements of the cervical spine compared to individuals who do not have the same condition, and this difference is significantly present for the flexion movement.
Keywords: Temporomandibular Disorder; isometric contraction; flexor strength; extenders.
Resumo: Introdução: A literatura aponta que indivíduos com Disfunção temporomandibular (DTM) também apresentam dor e alteração da postura da coluna cervical, porém ainda são escassos os estudos que tenham avaliado a força dos músculos cervicais. Objetivos: Avaliar a força muscular cervical em adultos jovens com e sem Disfunção temporomandibular. Materiais e Métodos: Participaram deste estudo, adultos jovens de 18 a 25 anos de uma universidade particular, com e sem diagnóstico de DTM e em bom estado geral de saúde. Foram excluídos os indivíduos com trauma no pescoço/cabeça; hérnia e degeneração discal; doenças sistêmicas como fibromialgia, lúpus; gravidez; bloqueio anestésico durante os últimos 3 meses. Foram aplicados questionários com dados gerais, Índice Anamnésico de Fonseca para avaliar os sinais e sintomas de DTM e Neck Disability Index (NDI) para avaliar o nível de incapacidade relacionado a dor na coluna cervical. A avaliação da força muscular dos músculos flexores e extensores da cervical mensurada pela contração voluntária isométrica máxima (CIVM) foi realizada utilizando-se de dinamômetro manual, modelo 2201163, Lafayette, IN, USA. Resultados: Foi observado maior frequência de sinais e sintomas de DTM moderada (53%). Foi identificado redução da força dos músculos do grupo DTM em relação ao grupo sem DTM para todos os movimentos, porém foi observada diferença significativa somente no movimento de flexão. Conclusão: Indivíduos com DTM apresentam menor força muscular para todos os movimentos da coluna cervical em comparação com indivíduos que não apresentam a mesma condição, sendo que essa diferença se apresenta de forma significativa para o movimento de flexão.
Palavras-chave: Disfunção Temporomandibular; contração isométrica; força flexores; extensores;
Recebido em 15 de Janeiro de 2024
Aceito em 27 de março de 2024
Introduction
The American Academy of Orofacial Pain (American Academy of Orofacia Pain) defined temporomandibular dysfunction (TMD) as clinical conditions that affect the chewing muscles, the temporomandibular joint and associated structures, which can cause various clinical manifestations in the individual (MACHADO et al; 2010).
Its etiology is multifactorial, and may be related to musculoskeletal changes, parafunctional behaviors, articular disc displacement, inflammatory autoimmune conditions such as ankylosing spondylitis and rheumatoid arthritis, malocclusion, postural changes, psychosocial problems and trauma (LOMAS et al., 2018).
Epidemiological studies show that between 50% and 75% of the general population present some sign or symptom of TMD (TODIC et al., 2019) The literature showed that, regarding the distribution between genders, TMD occurs more in women than in men (FERREIRA, 2016).
TMJ pain, joint noise, limited mouth opening, otalgia, jaw pain, toothache, bruxism, facial pain, tension-type headache and neck pain were the main complaints reported by patients with temporomandibular disorders (CAMACHO; WALDEMARIN; BARBIN; 2021).
Studies have shown that TMJ disorders can be associated with emotional suffering and multiple comorbidities related to central sensitization which, in turn, is responsible for producing hypersensitivity to pain, altering the sensory response. The pathophysiology of central sensitization in TMJ disorders is not yet well explained, however, there is a decrease in the pressure pain threshold after receiving mechanical stimuli (CAMPI et al., 2020).
Craniocervical imbalance is associated with the functionality of the anterior muscles (masseter, suprahyoid, sternocleidomastoid, longus head and neck muscle) and posterior muscles (trapezius, splenius, longissimus head and neck), passing imbalances and tensions between them (CORRÊA; BÉRZIN, 2004). Furthermore, the sternocleidomastoid muscle has the auxiliary function of supporting and stabilizing the head and cervical region and its coactivation during teeth clenching varies between 3 and 10% of the maximum voluntary contraction force (GIANNAKOPOULOS NN et al., 2013).
There is a stabilization pattern adapted for the head-neck segment. This pattern is based on the modulation of muscular activity to produce a constant stiffness value. Cervical flexor fatigue increases the participation of antagonist muscles, 99to counterbalance the effects of fatigue, motor adaptation adapts the net involvement of agonist and antagonist muscles to maintain the segment’s stiffness parameters at a constant level (PORTERO R et al., 2015).
There is evidence that TMD may be related to a decrease in the resistance of the cervical muscles (ARMIJO-OLIVO S, 2012). Given this, changes in body posture may be associated with a large number of disorders, including painful syndromes (Ferreira EAG et al., 2010), such as migraines and musculoskeletal disorders, such as temporomandibular dysfunction (FERREIRA et al., 2014)
The application of a protocol to assess the strength of peripheral muscles was highly successful, the assessment was carried out in a private and appropriate location. Isometric contraction was tested for the main movements of the largest joints of the upper muscles of the dominant limb. Before the assessment, the individual was guided and trained for each movement, after which the isometric contraction was performed for three seconds, the equipment always signaled the end evaluation for each movement. Each movement was performed three times, with the highest result of the three values being considered (JUNIOR BRVN; NETO MG, 2020).
The assessment of isometric muscle strength was carried out using the DHH, model 01165, from Lafayette Instrument, as well as an ISP goniometer, to adequately mark the joint position in the test of each muscle group (FIESELER et al., 2015).
We hypothesize that individuals with temporomandibular disorder have lower cervical muscle strength compared to control individuals. Given this, the present study aimed to evaluate cervical muscle strength in young adults with and without TMD.
Materials and methods
The present study is cross-sectional, analytical in nature. Young adults aged 18 to 25 from a private university, with a diagnosis of TMD and without a diagnosis of TMD, participated in this study. Individuals with neck/head trauma were excluded from this study; disc herniation and degeneration; systemic diseases such as fibromyalgia, lupus; pregnancy; anesthetic block during the last 3 months.
Initially, a questionnaire prepared by the author himself was applied with general data such as gender, age, weight, height, education, place of birth, marital status.
The Fonseca Anamnestic Index questionnaire was also applied to evaluate the signs and symptoms of TMD (FONSECA et al, 1994), this was translated and validated into Portuguese and has 10 questions, which allow answers, yes, no and sometimes , for which three scores are assigned 10, 0 and 5 respectively, which allow the volunteers to be classified into symptom severity categories: no TMD (0 to 15 points), mild TMD (20 to 45 points), moderate TMD (50 to 60 points) and severe TMD (70 to 100 points). For this study, the cutoff point adopted by Bertin et al, 2015 will be considered, therefore only individuals who have a score of 50 points or more will make up the group with TMD.
To assess the level of disability related to pain in the cervical spine, the self-administered Neck questionnaire was applied. Disability Index, a highly reliable instrument, already translated into Portuguese and widely used for self-reporting disability due to neck pain (VERNON, 2008; MCCARTY et al., 2007; COOK et al., 2006), this is a questionnaire composed of 10 questions related to the interference that neck pain causes in the patient’s most common activities of daily living ( ADLs ), the questions present six answer options, from no difficulty in the activity to intense difficulty.
Muscle strength
cervical flexor, extensor and lateral incline muscles measured by maximal isometric voluntary contraction ( MVIC) was carried out using a manual dynamometer ( Lafayette Instrument Company ®), model ٢٢٠١١٦٣, Lafayette, IN, USA (FIGURE I).

Figure I : Strength dynamometer
Source: Google Images
The dynamometer was attached to a belt made of inelastic material in order to avoid possible external forces that the examiner could generate, as previously described by FLORENCIO et al, 2015.
The peak force time, which is the time needed to reach maximum force in seconds of each contraction, was collected during the three repetitions of each task. Before capturing the signal, the patient performed a submaximal contraction, in order to familiarize himself with the task (LODOVICHE, 2018).
For the cervical spine flexion muscle strength, the volunteer was positioned in the supine position, knees and hips extended with the Velcro® belts placed firmly, one crossing the pelvis, and the other on the trunk, in order to reduce muscular movements and compensations during the task. Finally, the dynamometer was positioned on an imaginary midline, over the frontal bone. An MVIC was then requested by applying force against the dynamometer supported by the evaluator with instructions not to elevate the head, neck or chin (LODOVICHE, 2018).
For the muscular strength of cervical spine extension, the volunteer was positioned in the prone position, with Velcro® belts placed firmly across the pelvis and trunk. Finally, the dynamometer was positioned on an imaginary midline over the occipital bone. An MVIC was requested by applying a force against the dynamometer supported by the evaluator with guidance to avoid head and neck extension.
For the cervical lateral tilt contraction, the individuals were positioned in lateral decubitus, with their arms beside the trunk, with Velcro belts placed firmly at the greater trochanter and T3 levels. A height-adjustable pillow was placed to maintain the neck and head in a neutral position in the sagittal plane. The HHD was positioned in the temporal bone, 2 cm above the ear of the helix (FIGURE II).

Figure II: Position for strength measurements with a portable dynamometer adapted for maximal isometric contractions in the directions of cervical flexion, cervical extension and cervical lateral inclination.
The MVIC for flexion, extension and right and left bending will be performed in three repetitions of three seconds each, with a 20-second rest interval between each repetition, and three minutes between each task. The examiner used verbal commands to initiate and stimulate contractions and repetitions. The average value of the maximum voluntary isometric force generated from the three repetitions for each movement (flexion and extension) was used for comparison purposes. Peak force was collected in the kgf unit, all values were converted to Newton units (N) and normalized by the individual’s body mass, using the following formula: (manual dynamometer value (kgf).9.81/body weight) (LODOVICHE, 2018).
Quantitative variables were described by mean and standard deviation (mean ± SD) and qualitative variables were presented in frequency. The data were analyzed using the Statistical software Package for the Social Sciences (SPSS 18.0). The difference in mean angles between groups was compared using analysis of variance (ANOVA). The statistical significance level of p≤ 0.05 was adopted.
This Study was approved by the Research Ethics Committee of the CEUMA University, opinion nº 4,874,439 and All participants in this study signed the Free and Informed Consent Form.
Results
64 students were evaluated, with n=34 (53.12%) from the group with TMD and n=30 (46.88%) without TMD, with n=62 (96.87%) from the Physiotherapy course; n=1 (1.5%) from the Physical Education course and n=1 (1.5%) from the Biomedicine course; n=58 (90.62%) with single marital status and n=6 (9.38%) with married marital status; in the TMD group, n=29 (85.30%) were female and in the control group, n=23 (76.66%) were female, as can be seen in table I.
|
Variables |
Average |
DP |
P value |
|---|---|---|---|
|
Age years) |
|||
|
DTM Group |
20.97 |
2.38 |
P=0.94 |
|
Group control |
22.03 |
0.34 |
|
|
Weight (kg) |
|||
|
DTM Group |
59.81 |
12.43 |
P=0.64 |
|
Group control |
60.00 |
13.47 |
|
|
Height (m) |
P=0.87 |
||
|
DTM Group |
1.64 |
0.09 |
|
|
Group control |
1.64 |
0.10 |
|
|
BMI |
|||
|
DTM Group |
22.30 |
3.99 |
P=0.78 |
|
Group control |
22.35 |
4.17 |
Table I: Socio-demographic data of the group with TMD (n=34) and control group (n=30).
Regarding disability related to neck pain, it was found that in the total sample only 15 people reported having neck pain, being from the TMD group n=4 (11.76%) with mild disability and n=4 (11.76%) with moderate disability; from the control group n=5 (16.66%) with mild disability and n=2 (6.66%) with moderate disability.
In relation to the signs and symptoms of temporomandibular dysfunction, it was observed that N=20 (67%) of the control group received a mild severity level with a mean and SD of 32/9.27, in relation to the TMD group the moderate severity level was the most frequent, as can be seen in figure III.
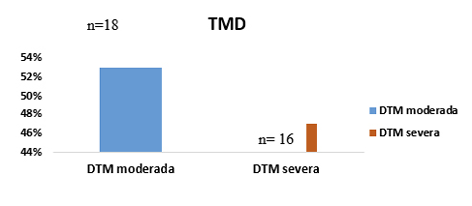
Figure III . Severity of temporomandibular disorder (TMD) n=34
A reduction in muscle strength was identified in all movements evaluated in the TMD group in relation to the control group, but a significant difference was observed only in the flexion movement. As can be seen in table II.
|
Variables |
DTM Group |
Group control |
P Value |
|
Flexion |
5.08±0.41 |
6.05±0.72 |
P=0.04* |
|
Extension |
7.11±1.23 |
7.87±1.2 |
P=0.64 |
|
Right Tilt |
5.66±1.23 |
6.70±0.88 |
P=0.52 |
|
Left Tilt |
6.26±1.25 |
6.76±0.7 |
P=0.71 |
*p<0.05
Table II: Average It is Detour standard from the strength of the muscles from the column cervical of the groups DTM n =34 and Control n=30
Discussion
In the present study, it was observed that TMD has a higher prevalence in females compared to males, which is in line with data found in the literature (MORENO et al., 2021).
Therefore , the higher prevalence in females may be related to the fact that women tend to seek treatment more frequently, being more careful and attentive to their health compared to men (PINTO, LEITE, SAMPAIO, & SANCHEZ, 2017) , in addition to hormonal changes during the menstrual cycle and stress may explain the high incidence in females (VASCONCELOS ET AL., 2019; TENREIRO E SANTOS; 2011).
The sample of this study was mainly composed of physiotherapy students , height and weight had homogenous results in both groups with an average age of 20 and 22 years, similar to the sample by Silva and Gonçalves (2022), in which students had an average age of 22 years in females.
Regarding the degree of severity of TMD, the highest prevalence was moderate TMD, similar data were found in studies by Silva et al. (2014), where the sample of most individuals was Moderate and severe TMD .
A small percentage of individuals were identified with some disability related to neck pain, findings that are in line with the study by Líbera et al. (2022) where 58.1% of the individuals participating in their study reported having neck pain. This difference in results can be explained by the difference in average age, which is higher, therefore, they have more years of illness, and the group in this study, being young, does not.
In this study, a difference was observed in MVIC between the groups with and without TMD for all movements evaluated with a significant difference for the flexion movement, suggesting that the presence of altered muscular performance in the cervical region may be related to the presence of the TMD condition and not necessarily to conditions related to pain in the neck. cervical spine, since in this study the groups homogeneously presented a small portion of individuals with neck pain with mild disability in the majority.
To the best of our knowledge, this is the first study that evaluates maximum contraction strength in individuals whose main pathology is TMD. In a previous study, Silva and Gonçalves (2022) evaluated individuals with TMD and headache in the same age group and with the same equipment used in this study and found a reduction in maximum contraction strength for the movements evaluated. Analyzing the results of these two studies, it can be suggested that TMD has as much influence as headache in reducing cervical spine muscle strength.
In contrast, Armijo -Olivo et al. (2010) found no significant difference between the maximum strength of the cervical flexor and extensor muscles in individuals with TMD and asymptomatic individuals. This divergence between the results can be explained by the methodological difference, since different devices were used to assess the strength of the muscles. Cervical.
In fact, it has been shown that individuals with TMD have reduced muscle strength without the presence of neck pain, which draws our attention since pain in the cervical region can be an aggravating factor for the decrease in muscle strength in this region. Our hypothesis is that TMD itself, as well as other chronic diseases, such as headache, for example, can alter muscle strength, without the presence of another comorbidity.
In view of the results of this study, attention is drawn to the assessment of muscle strength in individuals with TMD even if they do not have pain in the cervical region, in addition to promoting knowledge for physiotherapeutic professionals to develop the best intervention since physiotherapeutic treatment contributes for the prevention and remission of pain conditions, in addition to ensuring quality of life, through kinesiotherapy, myofasci al release and electrothermophotherapy .
This study has limitations in showing similar results, as not many articles were found in the literature with the same methodology and form of assessment, but the adoption of tools such as the Fonseca Anamnestic Index validated for Portuguese for assessment stands out as strong points. of signs and symptoms of TMD, and the manual dynamometer ( Lafayette Instrument Company ) to assess muscle strength.
Conclusion
The following research found that individuals with TMD have lower muscle strength for all movements of the cervical spine compared to individuals who do not have the same condition, with this difference being significant only for the flexion movement. We emphasize that this study complements the data available in the literature, in addition to producing knowledge for the scientific community that can benefit from this study.
REFERENCES
Arezes, P. M., Baptista, J. S., Barroso, M. P., Carneiro, P., Cordeiro, P., Costa, N., ... & Perestrelo, G. (Eds.). (2013). Occupational Safety and Hygiene (pp. ٣٢٧-٣٩٥). CRC Press.
Armijo-Olivo, S., Silvestre, R. A., Fuentes, J. P., da Costa, B. R., Major, P. W., Warren, S., ... & Magee, D. J. (2012). Patients with temporomandibular disorders have increased fatigability of the cervical extensor muscles. The Clinical journal of pain, 28(1), 55-64.
Benatto, M. T., Florencio, L. L., Bragatto, M. M., Lodovichi, S. S., Dach, F., & Bevilaqua-Grossi, D. (2019). Extensor/flexor ratio of neck muscle strength and electromyographic activity of individuals with migraine: a cross-sectional study. European Spine Journal, 28, 2311-2318
Camacho, G. B., Waldemarin, R. D. A., & Barbin, E. L. (2021). Temporomandibular disorder in adults: retrospective study. BrJP, 4, 310-315. DOI 10.5935/2595-0118.20210052
Campi, L. B., Visscher, C. M., Ongaro, P. C. J., Braido, G. V. D. V., Fernandes, G., & Gonçalves, D. A. G. (2020). Widespread Pain and Central Sensitization in Adolescents with Signs of Painful Temporomandibular Disorders. Journal of Oral & Facial Pain & Headache, 34(1). DOI 10.11607/ofph.2288
Cook, C., Richardson, J. K., Braga, L., Menezes, A., Soler, X., Kume, P., ... & Pietrobon, R. (2006). Cross-cultural adaptation and validation of the Brazilian Portuguese version of the Neck Disability Index and Neck Pain and Disability Scale. Spine, 31(14), 1621-1627. DOI: 10.1097/01.brs.0000221989.53069.16
Dos Santos Berni, K. C., Dibai-Filho, A. V., & Rodrigues-Bigaton, D. (2015). Accuracy of the Fonseca anamnestic index in the identification of myogenous temporomandibular disorder in female community cases. Journal of bodywork and movement therapies, 19(3), 404-409.
Fieseler, G., Molitor, T., Irlenbusch, L., Delank, K. S., Laudner, K. G., Hermassi, S., & Schwesig, R. (2015). Intrarater reliability of goniometry and hand-held dynamometry for shoulder and elbow examinations in female team handball athletes and asymptomatic volunteers. Archives of orthopaedic and trauma surgery, 135, 1719-1726.
Fonseca, M. D., Bonfate, G., Valle, A. L., & Freitas, S. F. T. (1994). Diagnosis by anamnesis of craniomandibular dysfunction. Rev Gaucha Odontol, 4(1), 23-32.
Giannakopoulos, N. N., Hellmann, D., Schmitter, M., Krüger, B., Hauser, T., & Schindler, H. J. (2013). Neuromuscular interaction of jaw and neck muscles during jaw clenching. J Orofac Pain, 27(1), 61-71.
LÍBERA, J. D., NAKANO, B. M. B., GUIOTTI, A. M., RODRIGUES, J. V. S., BRANDINI, D. A., DEVIDES, E. G. D. F., ... & TURCIO, K. H. L. (2023). Cervical muscle pain in patients with TMD and its correlations. Revista de Odontologia da UNESP, 51. DOI: https://doi.org/10.1590/1807-2577.04822
Lomas, J. (2018). Temporomandibular dysfunction. Australian journal of general practice, 47(4), 212-215.
Machado, I. M., Pialarissi, P. R., Minici, T. D., Rotondi, J., & Ferreira, L. P. (2010). Relation of the otological symptoms in the temporomandibular dysfunctions. Arquivos Internacionais de Otorrinolaringologia, 14(03), 274-279. DOI: 10.1590/S1809-48722010000300002
Moreno, A. G. U. T., Bezerra, A. G. V., Alves-Silva, E. G., Melo, E. L. D., Gerbi, M. E. M. D. M., Bispo, M. E. A., ... & Menezes, M. R. A. D. (2021). Influence of estrogen on pain modulation in temporomandibular disorder and its prevalence in females: an integrative review. DOI: https://doi.org/10.33448/rsd-v10i2.12453
Musto, F., Rosati, R., Sforza, C., Toma, M., & Dellavia, C. (2017). Standardised surface electromyography allows effective submental muscles assessment. Journal of Electromyography and Kinesiology, 34, 1-5.
Portero, R., Quaine, F., Cahouet, V., Léouffre, M., Serviere, C., & Portero, P. (2015). Influence of cervical muscle fatigue on musculo-tendinous stiffness of the head-neck segment during cervical flexion. PloS one, 10(9), e0139333. DOI: 10.1371/journal.pone.0139333
Tavares, L. F., Gadotti, I. C., Ferreira, L. M., Maciel, A. C. C., Carvalho, B. G., Barbosa, G. S., ... & Ribeiro, K. F. (2023). Pain, deep neck flexors performance, disability, and head posture in individuals with temporomandibular disorder with and without otological complaints. Journal of Back and Musculoskeletal Rehabilitation, (Preprint), 1-11. DOI: 10.3233/BMR-220079
1 Graduanda em Fisioterapia pela Universidade Ceuma, Campus Renascença, São Luís – MA, Brasil; e-mail: thayllane028204@ceuma.com.br ,ORCID: https://orcid.org/0009-0002-9394-2891; Autor Correspondente.
2 Doutora, Universidade Ceuma, Campus Renascença, São Luís – MA, Brasil , email: danielabassifisio@gmail.com, ORCID: http://orcid.org/0000-0002-6140-0177
3 Graduanda em Fisioterapia pela Universidade Ceuma, Campus Renascença, São Luís – MA, Brasil; e-mail: josmayarac@gmail.com, ORCID: https://orcid.org/0009-0008-1037-3536
4 Graduanda em Fisioterapia pela Universidade Ceuma, Campus Renascença, São Luís – MA, Brasil; e-mail: liviaanalima16@outlool.com, ORCID: https://orcid.org/0009-0008-1037-3536
5 Graduanda em Fisioterapia pela Universidade Ceuma, Campus Renascença, São Luís – MA, Brasil; e-mail: camilamoraescosta18@gmail.com, ORCID: orcid.org/0009-0001-7277-2400
6 Mestra no Programa de Pós-Graduação de Mestrando em Meio Ambiente da Universidade Ceuma, Campus Renascença, São Luís – MA; e-mail: kel.pinho7@gmail.com, ORCID: https://orcid.org/0000-0002-4119-0301
7 Mestranda no Programa de Pós-Graduação de Mestrando em Meio Ambiente da Universidade Ceuma, Campus Renascença, São Luís – MA; e-mail: maryticife@gmail.com, ORCID: 0009-0004-0575-3308
8 Doutora, Universidade Ceuma, Campus Renascença, São Luís – MA, Brasil , email: mcgfisio0@gmail.com, ORCID: 0000-0001-6457-2794